 Making dental restorations on a computer requires a huge leap of faith primarily by the provider of the service…your dentist. There can be no doubt the recipient of the service…..you (the consumer, client or what used to be called patient) rejoices with the new technology. No more messy gross impressions with bitter tasting gooey material that makes you want to vomit. Hallelujah and….very cool. No more two to three week long waits for a definitive restorations to be made. It almost makes going to the dentist fun…..well maybe thats a slight exaggeration.
Making dental restorations on a computer requires a huge leap of faith primarily by the provider of the service…your dentist. There can be no doubt the recipient of the service…..you (the consumer, client or what used to be called patient) rejoices with the new technology. No more messy gross impressions with bitter tasting gooey material that makes you want to vomit. Hallelujah and….very cool. No more two to three week long waits for a definitive restorations to be made. It almost makes going to the dentist fun…..well maybe thats a slight exaggeration.
But for your primary dental care provider, in order for digital dentistry to be considered a clear advantage it must include three things:
1 – Improved efficiency — both cost and time
2 – Improved accuracy in comparison to previous methods
3 – A high level of predictability of outcomes
“The major limitation of most areas of digital dentistry is cost. To adopt new technology often requires a higher capital investment, especially at the “innovator” or “early adopter” stage. Despite this, if the new technology meets the above criteria to be considered an advantage, then return on investment can be high if properly implemented.” 1
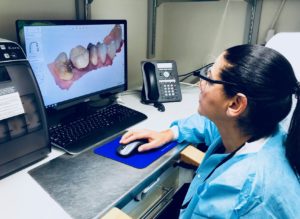
In 2018 we can all agree that efficiency, accuracy and predictability can be superior using digital scanners to capture intra-oral impressions and fabricate computer generated restorations……but here’s the caveat. Dentistry is plagued by the same limitations that surround every new technology in every industry….the technology is only as good as the people that work the software. Scanning a tooth and manufacturing a dental restoration involves little more than holding a wand in someone’s mouth and pushing a button once the restoration has been designed. The talent lies in designing the restoration on the CAD software.
“One of the common pitfalls in adopting new dental technology is lack of desire on the part of the clinician and team to be adequately trained. Some clinicians will purchase a new technology, yet never read the owner’s manual or seek advanced training on how to operate the technology efficiently, often leading to high failure and abandonment. Misunderstanding the new technology tends to foster slower adoption rates. This scenario can be easily avoided by greater attendance of basic and advanced hands-on courses in these areas of technology — not just the state’s minimum to maintain the dental license.” 2
Most dental practices will scan a tooth then push a button and the file is sent to a dental laboratory that designs the restoration and mills it within one to two days. The restoration is returned in a small plastic box and the dentist is left to insert the restoration without the luxury of having an analog cast to check the fit and precision of the margins. Essentially the dentist has no way to verify the accuracy or quality of the restoration until it is tried into the mouth….. and research has shown that it is much harder to gauge the accuracy of a dental restoration in the mouth compared to checking it on an analog cast……..unless that is…..you have a dedicated in office dental/computer engineer trained to use the design software.
Therein lies the dilemma. Unless a dental office hires a dental design software technician they must delegate the technique sensitive aspect of restoration design to an outside laboratory thus eliminating any quality control the dentist has over the making of the restoration.
Hiring the technician is a huge additional expense not to mention the cost of the design software, licensing fees and software updates. Some dentists that are computer savvy and enjoy the design aspect and control they achieve by investing in the design software will do it themselves but the majority of dentists have little time or interest and therefore delegate the work to an outside dental laboratory.
The message to the recipients of teeth made from this new technology? Have some knowledge about the process by which your dental restoration is being made and don’t be afraid to ask who is making it.
Kenneth M. Schweitzer, DDS
Schweitzer & Schweitzer DDS